Healthcare
Workforce
Planning
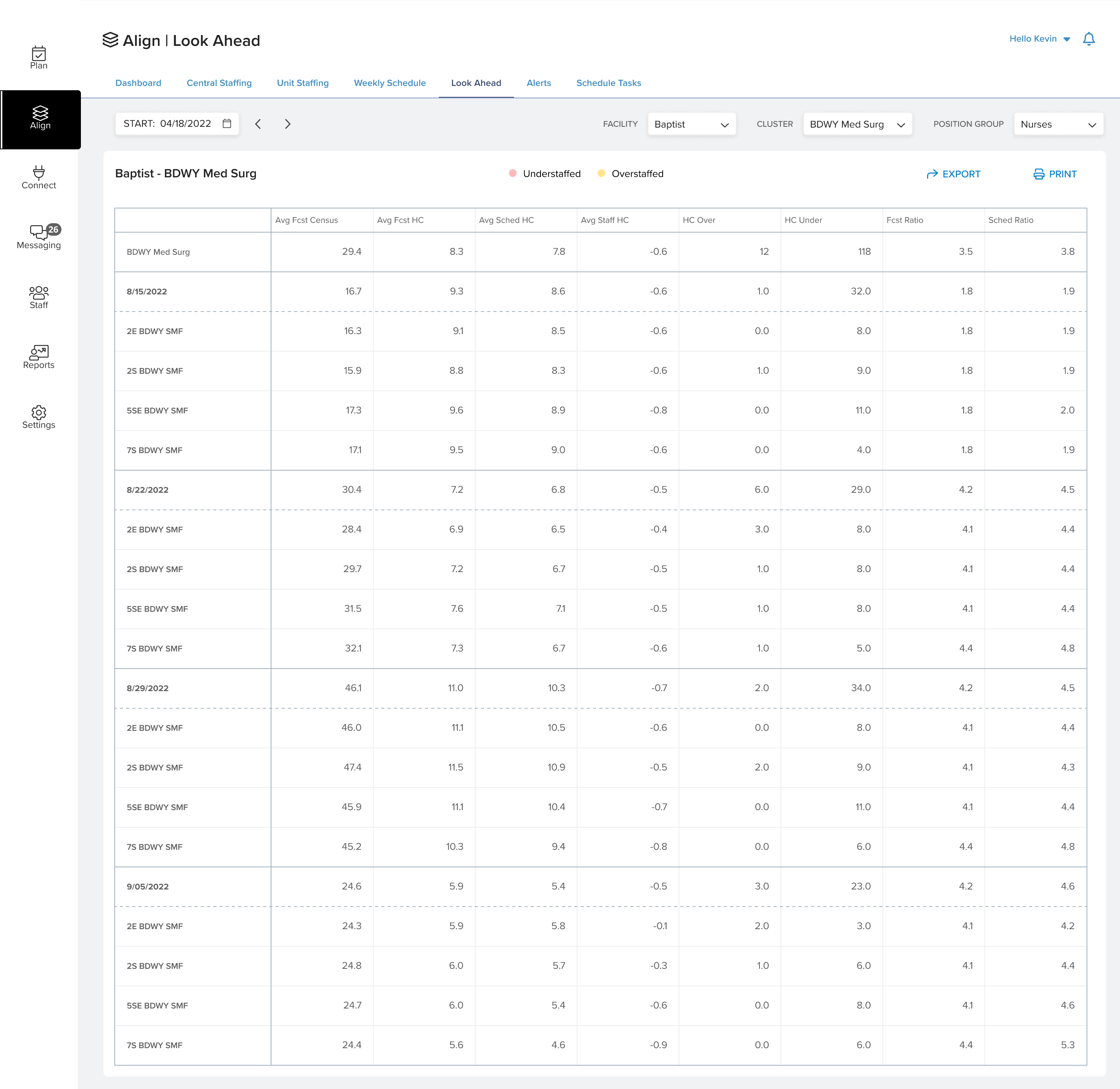
Flexwise was an existing healthcare workforce planning product with limited features and an established but underdeveloped framework. The engagement was a full rethink, with new features designed from scratch, existing features redesigned, and all of it held together within a consistent system language.
I led UX alongside an assistant UX and one additional UX designer, working with a team of four UI designers. My role sat upstream of execution: defining interaction architecture, writing feature definitions and experience documentation, guiding token and component structure to enable reusable animations and consistent patterns, and participating in client sessions to understand where the existing product was failing the people using it.
The platform served both executive decision-makers and operational planners across large hospital chains. These were organizations running 25–150 facilities, with 50–150 users per hospital. The user base numbered in the hundreds. The product was sold shortly after my contract concluded.